CHAPTER I
INTRODUCTION
I. 1 OVERVIEW
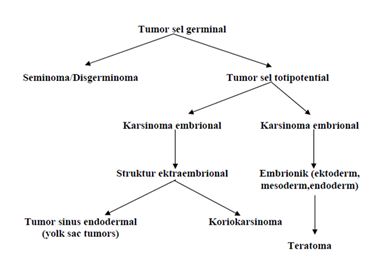
Teratomas are germ cell tumors are generally composed of multiple cell types derived from one or more of the three germ layers of endoderm, mesoderm and ectoderm. Inconsistent nomenclature is often confused about the various subtypes of teratoma. Teratomas derived from the Greek meaning of the terrace monster, which was first described by Virchow in the first edition of his book published in 1863. Teratoma is divided into three categories: mature teratoma (benign), immature teratoma and teratoma with differentiation monodermal particular degrees depending on the quantity of immature tissue showed the potential for malignancy. Cystic teratomas are generally benign and malignant solid is. Teratomas vary from a benign form of the cystic lesions of well differentiated (mature) to form a solid and malignant (immature). Immature teratomas are malignant germ cell tumor to the three most common after disgerminoma and endodermal sinus tumor. In addition, there also have a specific component (usually squamous) who experienced malignant transformation, but are rarely found.
In 1831, Leblanc created the term dermoid cyst in the literature of veterinary medicine when he succeeded in removing skin lesions at the base of the skull resembles a horse. Both teratomas and dermoid, a term still used and are often used interchangeably. Implications of these elements behawa beginning to resemble the skin with a complementary structure composed of dermoid, whereas teratoma has no such limit. Dermoid now known as the trigeminal and contain various types of tissue.

In the group that distinguishes between them, is a dermoid tumor with a more regular arrangement, ie with a well differentiated ektodermal and mesodermal tissue surrounding the endodermal component. Teratomas, particularly solid teratoma, not in good order. Thus, the degree of the composition, degree of cellular differentiation, cystic structures differentiate between dermoid with teratoma.

cystic teratoma of the ovary that shows some kind of network

Mature cystic teratoma of the ovary with hair, sebaceous material, and thyroid tissue.
In the division tumor somewhat gray with the red bleeding and necrosis. The presence of hair can be found in 2/5 cases, rare teeth but the bones, cartilage and calcification is often found. Although the main component is a solid tumor, but the cystic part was always found.
CHAPTER II
REVIEW REFERENCES
II.1 TERATOMA
II. 1.1 DEFINITIONS
Teratomas are germ cell tumors are generally composed of multiple cell types derived from one or more of the three germ layers of endoderm, mesoderm, and ekktoderm. Teratomas derived from the Greek meaning monster terrace. Teratoma is divided into three categories: mature teratoma (benign), immature teratoma, and teratoma monodermal with specific differentiation. Teratomas vary from a benign form of the cystic lesions of well differentiated (mature) to form a solid and malignant (immature). Cystic teratomas are generally benign and malignant solid is.
Immature teratomas are malignant germ cell tumor to the three most common after disgerminoma and endodermal sinus tumor. In addition, there also have a specific component (usually squamous) who experienced malignant transformation, but are rarely found.
II.1.2 ETIOLOGY
The presence of teratoma has been recognized for centuries, during which the origin of the cause is still a speculation and debate. In the past people believed the cause was due to swallowing teeth and hair, the curse of the witch, bad dreams, or in connection with the devil. The theory most widely used today are saying parthenogenik teratomas from primordial germ cells. This theory is supported by the anatomical distribution of the tumor along the migration path of primordial germ cells from yolk sac to the primitive gonad. Linder and colleagues conducted a study of mature cystic teratoma of the ovary. They use advanced cytogenetic techniques to show that these tumors originate from germ cells and arise from a single germ cell after the first meiotic division.
Teratomas composed of various cell types parenkimal from more than one germinal layer and often comes from the third layer. These tumors are derived from totipotent cells, usually in the midline or paraxial. The most frequent location is the sacrococcygeal (57%). Because it comes from totipotent cells, so often found in the gonad glands (29%). So far, the location of the most common gonad is the ovary, followed by the testis. Teratoma cysts sometimes appear in sequestered midline embryonic cell rests and be in the mediastinum (7%), retroperitonial (4%), cervical (3%) and intracranial (3%). Cells differentiate according to the germinal layer, which consists of various tissues in the body, such as hair, teeth, fat, skin, muscle, and endocrine tissues.
II.1.4 EPIDEMIOLOGY
Frequency
Freksuensi 25% of germ cell tumors in women under 15 years of age with median age 19 years.
Sakrokoksigeal teratomas are common tumors in newborns, occurring in 1 birth between birth 20000-40000.
Mature teratoma cysts occur in 10-20% of ovarian malignancies. This tumor is an ovarian germ cell tumor and also the most common malignant tumors in patients under 20 years old. Meanwhile, cases of bilateral tumors occur in 8-14% of all cases.
Testicular tumor incidence in men is equal to 2.1 to 2.5 cases per 100,000 population. Germ cell tumors occur in 95% of testicular tumor after puberty, but benign testicular teratoma is rare, amounting to only 3-5% of total cases of germ cell tumor. Incidence of testicular tumors in prepubertal children is 0.5 to 2 cases per 100,000, with the percentage of 14-27% mature teratoma. This merupajan tumor germ cell tumors in both common in this population. Benign teratomas of the mediastinum are rare, ie 8% of all tumors in this region kasusu.
Teratoma sakrokoksigeal
Teratoma sakrokoksigeal often diagnosed in prenatal period, and complications can arise during the before and after birth. Outcome after antenatal diagnosis is worse than the post-natal diagnosis and serial surgery, with survival rates varying from 54-77%
Potential complications include polyhydramnios and uterine bleeding tumor, which causes anemia and nonimmune hydrops fetalis. When there are. Atrioventricular shunting occurs in the tumor, hydrops can be caused by high output cardiac failure.
The development of hydrops is a bad sign. If it develops after 30 weeks' gestation, the mortality rate of 25%. When it has found no hydrops, labor direkommendasikan soon as possible after lung maturity occurs. The development of hydrops before 30 weeks' gestation have a worse prognosis, with 93% mortality rate. Makin et al. reported that interventions during the antenatal treatment of fetal hidrop not improve the outcome with mortality rates of 6 of 7 cases (86%). Hidrop and prematurity are the two factors that cause death and prematurity.
Teratoma sakrokoksigeal postpartum morbidity is associated with congenital anomalies, the time of tumor, recurrence occurs, and intra and postoperative complications. Ten to twenty four percent sakrokoksigeal teratoma associated with other congenital anomalies, especially defects in the hindgut and cloaca, which exceeds the estimated 2.5% in the general population [14,15,3].
On one series of studies examining 57 cases of benign teratoma during periods of 40 years of an institution, 5 cases of recurrence were reported. In that case, only one case that does not require koksigektomi recurrence, and there is one case which was originally considered a benign tumor with immature components of embryonal carcinoma was found after the third excision. In this study, too, found 3 patients had postoperative wound infections and one patient had postoperative pneumonia. Overall survival rate was 95% and morbidity or mortality rates consistently over a period of 40 years of research.
In the more recent study, 26 patients diagnosed with benign teratoma. Seven of 20 patients with long-term follow-up has developed neuropathic bladder and bowel disorders [15]. A longitudinal cross-sectional study found residual symptoms in childhood, improve with time, while functional symptoms were reported in adulthood is the same as the general population and did not increase beyond the control group [16].
Ovarian teratoma
Complication of ovarian teratomas include torsion, rupture, infection, hemolytic anemia, and malignant degeneration
Torque is the major cause of morbidity, occurring in 3-11% of cases. Some studies show an increase in the size of the tumor take is associated with increased risk of torque [2.17].
Rupture of cystic teratoma is rare and may occur spontaneously or due to torque. Many studies report states that the incidence rate of rupture is less than 1% [2.1], although penelian by Ahan et al. reported that occurred in 2.5% of the 501 patients studied [18]. Rupture may occur suddenly, causing shock or hemorrhage with acute chemical peritonitis. Chronic cases may also occur, which will mneyebabkan granulomatous peritonitis. Prognosisi after the rupture is usually good, but often times lead to rupture of thick adhesions.
Infections are rare and occur less than 1-2% of cases. Coliform bacteria is an organism that is often involved [18, 17].
Autoimmune hemolytic anemia have been associated with mature cystic teratoma cases. In this case, the tumor led to recovery of expenses of these symptoms. Back to the theory that the mechanism of pathogenesis of this is that (1) the substance of which is a tumor antigen to the host, causing the formation of antibodies that cross react with host red blood cells, (2) the production of antibodies against the tumor that directly host red blood cells , (3) terlapisnya red blood cells by a substance that causes changes in tumor antigenicity of red blood cells. Within this scope, radiological imejing of the pelvis is required in case of hemolytic anemia refractory [19.20].
In the original form, the mature ovarian cystic teratomas are almost always benign, but approximately 0.2 to 2% of cases of malignant transformation in one of its components, which often are squamous cell. Prognosis of patients with malignant degeneration is generally bad, but depending on the stage and type of cells undergoing degeneration [2.21].
Testicular teratoma
Testicular teratoma occurs in children and adults, but the incidence and course of their illness are very different. Teratomas are composed of 38% pure germ cell tumors in infants and children, but only 2% only after puberty. In children, usually benign, while in adolescents and adults often have metastases [22.23]. Therefore, the absence of metastases in prepubertas case, the limited morbidity of surgery and postoperative complications.
During and after puberty, all teratomas are considered malignant because even mature teratomas (which are histologically mature components) may have metastasis to lymph nodes or elsewhere retroperitonial. Metastatic rate varies from 29-76%. Morbidity associated with the growth of the tumor, which can invade or mengobstruksi local structure, so it becomes resectable. Approximately 20% of patients experienced a relapse during the period of supervision [22].
Teratomas of the mediastinum
Mature teratomas of the mediastinum, a mediastinal germ cell tumor, is a benign lesion. These tumors have no malignant potential as observed in testicular teratoma and can be cured by resection alone surgikal. Because of the location of these lesions, it is often the source of morbidity associated with postoperative complications intraoperasi and [24].
Gender
Teratoma sakrokoksigeal common in women than men, with a ratio of 3-4:1 women than men. Most of the reports say there is no sexual predilection medastinal teratoma. Unless, testicular teratoma, teratoma occurs in 75-80% of women.
Age
The location of the teratoma associated with age.
• In infants and early children, the most frequent location is ekstragonadal, whereas teratoma after children generally occur in the gonads.
• ovarian cystic teratoma can occur at any age, although often in the reproductive period. Common incident at the age of 20-40 years.
• testicular teratoma can occur at any age but is more common in infancy and children. In adults, pure teratoma tetikular rare, only 2-3% of germ cell tumor.
Mediastinal teratomas can appear at any age but often at the age of 20-40 years.
II.1. 5 DIAGNOSIS
Anamnesa
• Sacrococcygeal Teratoma
Sacrococcygeal teratomas can be diagnosed antenatally during a routine ultrasound examination or when the mother appeared with clinical symptoms such as pregnancy size larger than gestational age or polyhydramnios.
They have not been diagnosed in the antenatal period showed two patterns .. The most common pattern in the newborn period, which is present with large tumors are generally benign prominent in the sacral area that looks after the birth. Patterns are more rarely, in newborns may only show asymmetrical or buttocks that occurs when aged 1 month to 4 years with a tumor presakral to reach the pelvis. Symptoms of bladder or bowel dysfunction may arise. The second group are at higher risk for malignancy.

Epignathus large teratomatous diagnosed by ultrasound.
• Ovarian Teratoma:Cystic teratoma of the ovary Matur often found incidentally on physical examination, radiographic examination, or during abdominal surgery. Mature cystic teratoma of the ovary is often asymptomatic. The symptoms may appear:
Abdominal pain is usually constant and range from mild to moderate. Acute torsion and rupture will usually cause severe pain.
a palpable mass or swelling
abnormal uterine bleeding. Presumably due to the disruption of hormone production, but no histologic evidence of that support.
Symptoms of the bladder, indigestion, and back pain but may rarely occur

A 12-cm cystic teratoma ovarian mature before excision.
Often uncul as a mass in the scrotum that is painless, except for the teratomas are experiencing torque. In most cases, firm or hard masses, no tenderness, and not transilluminate. . Hydrocele is often associated with teratoma in childhood. On examination, testicular enlargement is diffuse rather than nodular.

A carcinoma of the testis there is a mixture of cartilage blue with red and white tumor tissue. Microscopically composed of teratoma, but there are also areas of embryonal carcinoma
Often without symptoms. Symptoms, related to mechanical effects include chest pain, cough, dyspnea, or symptoms related to recurrent pneumonitis. Many patients present with respiratory findings, and a pathognomonic finding trichoptysis, or a cough productive of hair or sebaceous material issue may occur if the mass and related trakeobronkial. Another serious symptom is the superior vena cava syndrome or lipoid pneumonia. Mediastinal teratomas are sometimes found incidentally on examination of thoracic images.
Investigations
• Laboratory
Increased serum alpha-fetoprotein (AFP) and beta-human chorionic gonadotropin (HCG) levels may indicate malignancy.
• Radiology
Investigations for most of the radiographic teratoma, and almost the same although the location varies.
If the teratoma been recorded in the uterus, serial ultrasound examinations should be performed to monitor fetal hidropfetaliss kemngkinan occurrence. In the case of sacrococcygeal teratoma, ultrasound can demonstrate cystic components and extension of tumor into the pelvis or abdomen, as illustrated in the figure below. USG illustrates the shift vesica urinary and rectal, with compression of the ureter resulting in hydronephrosis or hydroureter

Epignathus teratoma
CT scan of abdomen and pelvis before surgical exploration may further describe the sacrococcygeal tumor.
Similar to ultrasound, adjuvant CT scan is useful in diagnosing ovarian teratoma and can detect the involvement of the liver and lymph kelenlar in malignant cases. In a study of transvaginal ultrasonography has a high to distinguish teratoma from other ovarian masses.
MRI can distinguish density and lipids in the blood and other fluids may be useful as an additional examination for the diagnosis of ovarian teratoma, with an accuracy of 99%.
In the case of a mediastinal teratoma dicurgai photo anterior-posterior thoracic and lateral dpat provide important information about the size and location of the mass. CT scan and / or MRI may further clarify the diagnosis and also very useful in describing the limits of mediastinal mass, the potential involvement of blood vessels, and honor.
Echocardiography can be used to describe the physiological effects of mediastinal masses, such as tamponade or pulmonary stenosis, and can be used to guide needle biopy. Fine needle biopsy can be used to differentiate benign and malignant mediastinal mass in 90% of cases.
• Histology
In teratomas, the exterior of the wall of the tumor is usually covered by the original network. Cyst cavity are lined with squamous epithelium and keratin usually contains many sebaceous and sweat glands. Hair and other appendages of skin usually appears. Sometimes, the cyst wall lined by bronchial or gastrointestinal epithelium. Giant-cell reaction can be seen in many tumors and may, in the case of intraperitoneal teratomas, caused extensive adhesion formation if the contents of tumor rupture. Ectodermal tissue may be found including the brain, glia, neural tissue, retina, choroids, and ganglia. Mesodermal tissue represented by bone, cartilage, smooth muscle and fibrous tissue.
II.1.6 STADIUM
In microscopic differentiation of the system used a modified Norris by Robboy and Scully:
Degree 0: Network-wide tumor
Degree 1: Most of the immature tissue, especially the ganglia. Mitosis can be found, but the neural epithelium is not found or limited to one field of view per slides
Grade 2: Most of the immature neural epithelium 1-3 slides per
Grade 3: Network with heavy immature neural epithelium of> 4 per slides and often resembling choriocarcinoma.
Department of Surgery of the American Academy of Pediatrics, Altman and colleagues report Sacrococcygeal teratoma type classification system as follows:
Type I: Most of the external tumor, attached to the tail bone, and may have a small presacral component (45.8%). No metastasis was associated with this group.
Type II: Tumor has both external mass and significant pelvic presacral extension (34%) and have a metastatic rate of 6%.
Type III: tumors visible from the outside, but the dominant mass is pelvic and intraabdominal (8.6%). 20% rate of metastasis was found in this group.
Type IV: lesions not visible from the outside but completely presacral (9.6%) and have a metastatic rate of 8%.
II.1.7 MANAGEMENT
Management of teratoma most surgical therapy.
Sacrococcygeal Teratoma
Sacrococcygeal teratoma diagnosed prenatally should be monitored closely.
Fetuses with larger tumors, surgery should be considered Sectio Caesarea to prevent dystocia or tumor rupture. Due to the poor prognosis associated with the development hidropfetalis before 30 weeks' gestation, the fetus is favorable for surgery when the uterus. In most cases, sacrococcygeal teratoma resection should be performed electif the first week of life, because the longer dituda can increase the level of malignancy.
Ovarian teratomas
Mature cystic teratoma of the ovary can be removed by simple cystectomy than salpingo-oophorectomy.
Although very rare malignant degeneration, the cyst must be removed in its entirety, and if immature elements are found, the patient must undergo a standard stage classification procedure.
Testicular teratoma
Testicular teratoma treated by simple or radical orchiectomy. More recently, conservative excision with enucleation have also been recommended in the prepubertas the testis. The risk of malignancy increases with maturation of the testis.
Teratomas of the mediastinum
Mature teratomas of the mediastinum should be resected. Tumor may be attached to the surrounding structures, which require resection of the pericardium, pleura, or lung. When complete resection can reduce the risk of recurrence.
II.2. Dermoid cyst
II.2.1 DEFINITION
Dermoid cyst a teratoma is a benign dalah where ektodermal structures with good differentiation, such as the epithelium of the skin, hair, teeth and sebaceous glands of the product resembles a yellow-white fat, appears to be more prominent than the elements of entoderm and mesoderm. This occurs because the tissue cysts in the egg is not fertilized. Then grow into tissues such as hair, bone and fat.
III.2.2 CHARACTERISTICS
There are no traits that are characteristic of dermoid cyst. Cyst wall appear grayish-white, and somewhat thin. Partially cystic tumor supple consistency, solid elsewhere. At first glance it looks like a hollow cyst, but when cleaved, usually appear one large cyst with a small room within the walls. In general, there is one area on the inner wall, a prominent and dense.

Tumors contain elements ektodermal, mesodermal, and entodermal. Then match the skin, hair, glands sebase, teeth, cartilage, muscle fibers of connective tissue, and gastrointestinal tract mucosa, respiratory epithelium, and thyroid tissue. Material contained in the cavity of the cyst is a product of the sebaceous glands in the form of soft masses just as fat, mixed with hair.

III.2.3 Symptoms
Cysts on both ovaries and can usually asymptomatic. Dermoid cysts can occur on the torque shaft with symptoms of sudden pain in the lower abdomen. Can also tear the wall of the cyst that resulted in evisceration cyst into the peritoneal cavity.
CHAPTER III
CONCLUSION
Teratomas are germ cell tumors are generally composed of multiple cell types derived from one or more of the three germ layers of endoderm, mesoderm and ectoderm. Dermoid cyst a teratoma is a benign dalah where ektodermal structures with good differentiation, such as the epithelium of the skin, hair, teeth and sebaceous glands of the product resembles a yellow-white fat, appears to be more prominent than the elements of entoderm and mesoderm.
Sacrococcygeal teratomas can be diagnosed on antenatal ultrasound examination during routine or when the mother appeared with clinical symptoms such as pregnancy size larger than gestational age or polyhydramnios. On ovarian and testicular teratomas are asymptomatic unless the tumor tertorsi or ruptures can cause pain. Whereas in mediastinal teratoma presenting symptoms, associated with the mechanical effects include chest pain, cough, dyspnea, or symptoms related to recurrent pneumonitis. Dermoid cysts often cause no symptoms unless the cyst ruptures tertorsi or that can cause pain.
The management of teratomas and dermoid cysts most surgical therapy. Complete removal of the tumor and both can reduce the risk of recurrence.
REFERENCES
1. Sjamsuhidajat R., Wim de Jong. Buku ajar Ilmu Bedah, Edisi II. Jakarta : EGC, 2004.
2. Mitchell R, Kumar Vinay. Et.al. Buku saku Dasar Patologis Penyakit, Edisi 7. Jkarta
3. Chad A Hamilton, MD. Cystic teratoma. Januari 2012. http://emedicine.medscape.com/article/281850-overview.
4. Robert A Schwartz, MD, MPH. Dermoid Cyst. Febuari 2012. http://emedicine.medscape.com/article/1112963-overview
5. Adkins E Stanton, MD. Pediatric Teratomas and Other Germ Cell Tumors Follow-up. Desember 2011. http://emedicine.medscape.com/article/939938-followup.
6. Dr. Herry Setya Yudha Utama, Sp.B MHKes FinaCS. Case Report and Literature Review: Fetus in Fetu Laki-laki Hamil Selama 4 tahun. November 2011. http://www.herryyudha.com/2011/11/case-report-and-literatur-review-fetus.html
No comments:
Post a Comment