CHAPTER I
INTRODUCTION
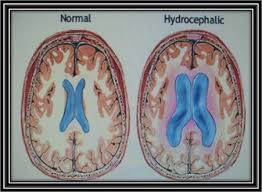
Hydrocephalus comes from hydro meaning water and chepalon which means head. Hydrocephalus is a buildup of cerebrospinal fluid (CSS) is actively causing dilatation of the ventricular system of the brain where there is excessive accumulation of CSF in one or more of the ventricles or subarachnoid space. This situation is caused because there is imbalance between production and absorption of the CSS. If the excessive accumulation of CSF occurs on the cerebral hemispheres, a condition called subdural higroma or subdural fluid collection. In the case of excessive fluid accumulation occurs in the ventricular system, a situation known as hydrocephalus internal.Selain that some intracranial lesions causing elevation of ICT, but not until the cause of hydrocephalus. CSS is not equivalent to raising the volume with hydrocephalus; it also occurs in cerebral atrophy.

Hydrocephalus as a clinical entity distinguished by three factors: a). Intraventrikuler pressure elevation, b). Addition of CSS volume, c). Dilatation of the cavity CSS. Overall, the incidence of hydrocephalus is estimated close to 1: 1000. while the incidence of congenital hydrocephalus varies for each of the different populations. BL Hershey said most of hydrocephalus in children is congenital is usually seen in infancy. If hydrocephalus appears after age 6 months is usually not because of congenital. Mujahid Anwar et al get 40-50% of infants with intraventricular hemorrhage grade 3 and 4 had hydrocephalus. Pongsakdi Visudiphan et al in a study 36 of 49 children with TB meningitis had hydrocephalus, with a second note 8 children with obstructive hydrocephalus and 26 children with communicating hydrocephalus. Hydrocephalus that occurs as a complication of bacterial meningitis can be found at any age, but more often in infants than children.
CHAPTER II
ANATOMY
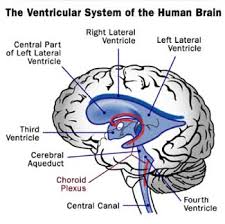
Anatomical structures associated with hydrocephalus, the buildings where the CSS is located. Ventricular system of the brain and central canal.

1. Lateral ventricle
There are two, located in the telencephalon hemispherii. The second related some of the lateral ventricle III ventricle (LV Tertius) through interventrikularis foramen (Monro).
2. III ventricle (ventricle Tertius)
Located in the diencephalon. Lateral wall is formed by the thalamus and hypothalamus with adhesio interthalamica. Infundibularis optic recess and protruding into the anterior, and the recess and the recess pinealis suprapinealis caudal direction. III ventricle associated with IV ventricle through a small hole, which is aquaductus Sylvii (aquaductus cerebri).
3. IV ventricle (ventricle Quartus)
Form a dome-shaped space above the fossa between the cerebellum and medulla rhomboidea and extending along the lateral recess on both sides. Each recess ends at the foramen Luschka, the mouth of the lateral ventricle IV. In the attachment there is a vellum medullare anterior median Apertura Magendie.
4. Central canal spinal cord and medulla oblongata
The central channel spinal cord: a small channel that extends along the spinal cord, coated ependimal cells. Above, continued into the medulla oblongata, where it opens into the fourth ventricle.
Subarakhnoidal space
Is the space that lies between the arachnoid layer and piamater.

CHAPTER III
Hydrocephalus
III.1. Pathophysiology
CSS generated by choroideus plexus of lateral ventricles and flows into the third ventricle, and from here through aquaductus into IV ventricle. There, the liquid entering the cerebrospinal liquor spatium externum through the foramen of the lateral and medial of the IV ventricle. CSS drainage into the venous circulation occurs partly through the villi arachnoidea, which protrude into the sinus venosus or into Lacuna laterales, and partly on the exit spiral cord, where the transition into the venous plexus and into the dense sheath of nerve-sheath ( a way to circulus lymphaticus).
CSS formation rates from 0.3 to 0.4 cc / min or between 0.2 - 0.5% of total volume per minute and there is a call between 14-38 cc / hour. Secretion of total CSS in 24 hours is about 500-600cc, while the total jumblah CSS is 150 cc, in a day means an exchange or renewal of the CSS as much as 4-5 times / day. In the total neonates jumblah CSS and will range from 20-50 cc increases with age until it reaches 150 cc in adults.
Hydrocephalus occurs arising from the imbalance between production and absorption and circulation disorders CSS.
Apart from interference with the production, absorption, and circulation, hydrocephalus can also arise due to: cerebral dysgenesis and cerebral atrophy.
III.2. Classification
Hydrocephalus can be classified on several things, among others:
A. Based on Anatomical / CSS to obstruction
• Hydrocephalus type of obstruction / non communicating
CSS occurs when the brain is interrupted (Disturbance in the ventricular system or the resulting blockage of the flow of CSS in the brain ventricular system), which is most commonly caused by congenital: Sylvius aqueduct stenosis (causing dilatation of the lateral ventricles and third ventricle. IV ventricle is usually normal in size and location ). Which is somewhat rare as a cause of hydrocephalus is Dandy-Walker syndrome, foramen of Monro atresia, congenital vascular malformations or tumors. Inflammation (exudate, meningeal infection). Bleeding / trauma (subdural hematoma). Tumor in the ventricular system (intraventrikuler tumor, parasellar tumors, tumors of the posterior fossa).
• type of communicating hydrocephalus
Rarely found. Occurs due to excessive or impaired absorption process (disturbance outside the ventricular system).
o Bleeding due to birth trauma causes adhesions and arachnoid villi causing blockade.
o Inflammation of meningeal
o Congenital:
Attachment arachnoid / sisterna due to disruption of the formation.
Impaired formation of arachnoid villi
plexus papilloma choroideus
2. Based on etiology:
A. Type of obstruction
a. Congenital
a.1.Stenosis cerebral aqueduct
Have various causes. Most are caused by infection or hemorrhage during fetal life; true congenital stenosis is very rare. (Toxoplasma / T.gondii, Rubella / German measles, X-linked hydrocephalus).
a.2.Sindrom Dandy-Walker
These malformations involving 2-4% of newborns with hydrocephalus. The aetiology is unknown. This form of expansion of cystic malformations IV ventricle and hypoplastic cerebellar vermis. Hydrocephalus that occurs due to the relationship between IV ventricular dilatation and inadequate subarachnoid cavity, and this may appear at birth, but 80% of cases are usually seen within the first 3 months. Such cases often occur in conjunction with other anomalies such as agenesis of the corpus callosum, labiopalatoskhisis, ocular anomalies, cardiac anomalies, and so forth.
Arnold-Chiari a.3.Malformasi
A rare congenital anomaly in which the two parts of the brain is the brain stem and cerebellum have an extension of normal size and protrude into the spinal canal
a.4.Aneurisma vein Galeni
Vascular damage that occurs at birth, but normally not be detected until a few months old. This happens because the vein of Galen Sylvii flows over the aqueduct, and form a pocket bulging aneurysm. Often the cause of hydrocephalus.
a.5.Hidrancephaly
A condition where the brain hemispheres are not replaced with a bag adadan CSS.
b. Acquired (Acquired)
b.1.Stenosis cerebral aqueduct (after infection or bleeding)
Meningitis is an infection by bacteria, causing inflammation of the membranes (meninges) surrounding the brain and spinal cord. Hydrocephalus develops when scar tissue blocks the flow of meningeal infection CSS in the subarachnoid space, through the aqueduct in the ventricular system or affect the absorption of CSS in the arachnoid villi. If time did not get treatment, bacterial meningitis can cause death within a few days. The signs and symptoms of meningitis include fever, headache, high fever, loss of appetite, stiff neck. In extreme cases, symptoms of meningitis are indicated by vomiting and seizures. Can be treated with high doses of antibiotics.
b.2.Herniasi supratentorial tumors due to tentorial
b.3.Hematoma intraventrikuler
If severe enough to affect the ventricles, causing blood to flow in the tissue surrounding the brain and cause neurological changes. The possibility of developing hydrocephalus by blockage or reduction sisebabkan brain's ability to absorb CSS.
b.4.Tumor (ventricle, vinialis region, posterior fossa)
The majority of brain tumors experienced by children at age 5-10 years. 70% of these tumors occur in the back of the brain called the posterior fossa. The other type of tumor is the brain that can cause hydrocephalus intraventrikuler tumor and is often the case choroideus plexus tumors (including papilloma and carsinoma). Tumors located in the back of the brain most will obstruct the flow of CSF out of the IV ventricle. In many cases, the best way to treat hydrocephalus associated with tumors is to remove the tumor causing the blockage.
b.5.Abses/granuloma
b.6.Kista arachnoid
Cysts are closed sacs soft or liquid-filled holes. If there arachnoid cyst is filled sac lined with a network CSS and the arachnoid membrane. Cysts are usually found in children and is in the brain ventricles or the subarachnoid space. Subarachnoid cysts can cause non communicating hydrocephalus by blocking the flow of CSS in the ventricles, especially ventricular III. Based on the location of cysts, neurosurgeons can remove the cyst wall and cyst fluid drain. If cysts are found in places that can not be operated on (near the brain stem), the doctor may put a shunt to drain the fluid to be absorbed. This will stop the growth of cysts and protect the brain stem.
3. Based on Age
o type of congenital hydrocephalus / infantile (baby)
o Hydrocephalus type juvenile / adult (children / adult)
In addition to the division based on the anatomy, etiology, and age, there are also types of Normal Pressure Hydrocephalus: as a convention, hidrosefalik syndrome, including signs and symptoms of exaltation of ICT, such as a large head with bulging fontanelle. Lately, reported clinical findings of hydrocephalus which does not coincide with the elevation of ICT. A person can be diagnosed with normal pressure hydrocephalus have an enlarged brain ventricles, but there is little or no increase in ventricular pressure. Typically experienced by elderly patients, and is largely due to impaired CSF flow and abnormal brain compliance.
In adults may arise "normal pressure hydrocephalus" as a result of: a). Subarachnoid hemorrhage, b). Meningitis, c). Head trauma, and d). Idiopathic. With the triad of symptoms: a). Mental disorders (dementia), b). Interference coordination (ataxia), c). Urinary disorders (inkontinentia urine)
III.3. Clinical Overview
Clinical picture at the beginning of the enlargement of the skull which was followed by a neurologic disorder caused by an increased liquor pressure that causes the brain hipotrofi.
Hydrocephalus in infants (sutures still open at the age of less than 1 year) got the picture:
o Head of enlarged
o suture widened
o Fontanella prominent head
o eye towards the bottom (sunset phenomena)
o horizontal nystagmus
o Percussion head: "cracked pot sign" or like a ripe watermelon.
The average size head circumference

o Headache
o Awareness of decreased
o Restlessness
o Nausea, vomiting
o Hiperfleksi as increases tonus limb
o physical and mental disorders
o Papil edema; visual acuity will decline further and may lead to blindness if there is atrophy of the papillae N.II.
Raised intracranial pressure due to the crown and the suture is closed, headache especially in the bifrontal and bioksipital. Physical and mental activity will gradually decrease with a common mental disorders such as slow response to the environment, less attention was not able to plan their activities.
III.4. Examination and Diagnosis
• Clinical symptoms
• X Pictures head, obtained
o thin bones
o craniofacial disproportion
o suture widened
With this procedure can be known:
a. Types of congenital hydrocephalus / infantile
b.Hidrosefalus type of juvenile / adult: because sutures have closed the X-rays of the head of the picture is expected to rise in intracranial pressure.
• transillumination; spread of light beyond the light source over the limit, 2.5 cm frontal, occipital 1 cm
• Examination CSS. Aseptic manner via ventricular puncture / puncture fontanela mayor. Determine:
o Pressure
o Jumblah cells increases, suggesting an inflammatory / infectious
o The presence of erythrocytes showed bleeding
o If there is infection, was examined by culturing the bacteria and antibiotic sensitivity.
• ventriculography, ie by entering the contrast of pure O2 or other contrasting with a specific tool to penetrate through the anterior Fontanella directly into the ventricles. After contrast entered directly photographed, it will show the contrast filling the dilated ventricular chamber. Greater in children who have been shut down because fontanela ontuk memaukkan contrast with the drill holes made in the frontal or occipital karanium. Ventriculography is very difficult and have a high risk. In hospitals that have had a CT scan facility, this procedure has been abandoned.
• CT scan of the head
o The CT scan of obstructive hydrocephalus often show widening of the lateral ventricles and third ventricle. Can occur in the ventricle is larger than the occipital horns of the child. IV ventricle are normal in size and a decrease in the density due to reabsorption transependimal of CSS.
o In the communicant hydrocephalus CT scan image shows mild dilatation of the ventricular system, including all in the proximal subarachnoid space of the blockage.
Advantages CT scan:
a clearer picture
Non-traumatic
predict prognostic
The cause of hydrocephalus may be suspected
• USG
Performed through the anterior fontanela still open. With ultrasound is expected to show a widened ventricular system. Another opinion says an ultrasound examination in patients with hydrocephalus did not have value in determining the state of the ventricular system because it is caused by ultrasound can not describe the anatomy of the ventricular system are obvious, as in a CT scan.
III.5. Diagnoses
Higroma subdural; accumulation of fluid in the subdural space subdural hematoma due to liquefaction
subdural hematoma: accumulation of blood in the subdural cavity
Emfiema subdural; the presence of air or gas in the subdural tissue.
Hidranensefali; at all, or virtually no cerebral hemispheres, fill in the space normally filled hemispheres CSS
brain tumors
Head of
o Megaloensefali: increased brain tissue
o Makrosefali: bone disorders
In the diagnostic process, essential for expert diagnosis of neuro (nerve) and neuro surgery to determine the prognosis and therapeutics.
Complications of hydrocephalus:
1. Brain atrophy
2. Herniation of the brain that can result in death.
CHAPTER IV
MANAGEMENT
Therapy
Medical treatmentIntended to limit the evolution of hydrocephalus through efforts to reduce the secretion of fluid from the plexus khoroid or efforts to improve resorpsinya. Can be tried in patients who are not life threatening, especially in health centers where there is no means of surgical sarf.
Drugs are commonly used are:
Asetasolamid
Mode of administration and dosage: Per oral 2-3 x 125 mg / day, this dose may be increased to a maximum of 1,200 mg / day
Furosemide
Mode of administration and dosage: Per oral, 1.2 mg / kg iv injection 1x/day or 0.6 mg / kg / day if no change after a week of programmed patients for surgery.
Repeated lumbar punctures (serial lumbar puncture)
Repeated lumbar puncture mechanism to stop the progression of hydrocephalus in this case it is not certain. On repeated lumbar puncture the pressure drop will occur intermittently CSS which allows absorption by the villi arakhnoidalis CSS will be easier. Indications: generally done on communicant hydrocephalus, especially in hydrocephalus after subarachnoid hemorrhage, periventricular-intraventricular tuberculosis and meningitis. Also indicated the communicant hydrocephalus shunt which can not be done or is likely to occur herniation (impending herniation)

How to:
1. LP carried out by using 22-gauge needle, the interspace L2-3 or L3-4 and CSS allowed to flow under the influence of gravity.
2. LP is stopped when the flow stops CSS. But there is also a way to use CSS LP issued every 3-5 ml.
3. At first, LP done every day, if the CSS that came out less than 5 ml, LP diperjarang (2-3 days).
4. Evaluated with a CT scan of the head every week.
5. LP discontinued if persistent ventricular size on CT scan 3 weeks in a row.
6. This action is considered failed if:
persistent ventricular dilatation
Cortical thinner coat
In the lumbar puncture site occurred sikatriks
progressive ventricular dilatation
Complications: transtentorial herniation or tonsiler, infection, and electrolyte disturbances hipoproteinemia.
Therapy Operations
Surgery is usually done in patients with hydrocephalus directly. In patients awaiting emergency surgery are usually given:
Mannitol infusion of 0.5 to 2 per g / kg / day given in a period of 10-30 minutes.
1. "Third Ventrikulostomi" / III ventricle
Through kraniotom, III ventricle was opened through the khiasma optikum, with the aid of endoscopy. Subsequently made a hole so that the CSS of the III ventricle can flow out.
2. Bypass / "shunting"
There are two kinds:
External
CSS flow from the ventricle to the outside of the body, and is only temporary. For example: lumbar puncture repeated for normal pressure hydrocephalus therapy.
Internal
a. CSS flow from the ventricle into the other limb.
~ Ventrikulo-Sisternal, CSS applied to the sisterna magna (Thor-Kjeldsen)
~ Ventrikulo-Atrial, CSS applied to the right atrium.
~ Ventrikulo-Sinus, CSS superior sagittal sinus drained into
~ Ventrikulo-bronchial, CSS applied to the bronchi
~ Ventrikulo-Mediastinal, CSS applied to the mediastinum
~ Ventrikulo-peritoneal, CSS flowed into the peritoneal cavity
b. "Lumbo Peritoneal Shunt"
CSS flow of lumbar spinal Resessus into the peritoneal cavity with open surgery or with a percutaneous needle Touhy.
Complications of shunting
Infection
subdural hematoma
Obstruction
a low state of CSS
Ascites
Kraniosinostosis
REFERENCES
2. Atlas Berwarna & Teks Anatomi Manusia jilid 3, edisi 6, sistem saraf dan alat-alat sensoris. Kahle, Leonhardt, Platzer. (Hipokrates, hal 262-271)
3. KAMUS KEDOKTERAN DORLAND, Penerbit Buku Kedokteran EGC
4. http://emedicine.medscape.com/article/1135286-overview.
5. http://www.hydrocephalus.org/.
6. Anonim, 1996, Kelainan Neurologi Hidrosefalus dalam Harsono (editor) Buku Ajar Neurologi Klinis dan Kapita Selekta, Gadjah Mada University Press, Bulaksumur, Yogyakarta.
7. Anonim, 1985 Hidrosefalus dalam Hassan, R., Alatas, H. (editor) Kumpulan Kuliah Kesehatan Anak Fakultas Kedokteran Universitas Indonesia, cetakan ke IV, Jakarta.
8. BUKU AJAR ILMU BEDAH edisi 2, R.Sjamsuhidat, Wim deJong. EGC, Jakarta 2004. (hal 809-810)
9. ILMU BEDAH SARAF, Dr. Syaiful Saanin, Neurosurgeon, Ka.SMF Bedah Saraf RS. Dr. M. Djamil / FK-UNAND Padang.
10. Sjamsuhidajat. R, Jong WD, Hidrosefalus in Buku Ajar Ilmu Bedah, Edisi 2, Penerbit Buku Kedokteran EGC, Jakarta, 2004.
No comments:
Post a Comment