Malignant SKIN TUMOR AT AGLANCE
( Basal Cell Carcinoma, Squamous Cell Carcinoma, Malignant Melanoma )
Malignant skin tumor is a disease characterized by the growth of skin cells that are not controlled, can damage surrounding tissue and can spread to other parts of the body. Because the skin consists of several types of cells, the skin cancer also vary according to cell type affected.
Epidemiology
Adult skin cancer tend to have increased in number especially in the Americas, Australia and Britain. Based on several studies, those white people are more likely to suffer this type of skin cancer. It is predicted as a result of their frequent exposure (lots of exposure) sunlight. In Indonesia people with skin cancer is fairly small compared to the third-countries, however, skin cancer needs to be understood because in addition to causing defects (damage the appearance) is also at an advanced stage can be fatal to the patient (1).
Malignant skin tumor types that are found throughout the world are basal cell carcinoma (basalioma), squamous cell carcinoma, a relatively non melanoma and malignant melanoma. Basal cell carcinoma is the most common. In America, about 800,000 people suffering this cancer every year. 75% of skin cancer are basal cell kanser. Squamous cell carcinomas are found to be what the 200,000 Americans each year. Melanoma is the most rare but cause the most deaths. According to WHO, as many as 160,000 people suffering melanoma each year and as many as 48 000 deaths are reported each year (3).
Skin Embryology (4)
The skin has a double origin:
(A) the superficial layer (epidermis), formed from the surface ectoderm.
(B) inner layer (dermis), derived from the underlying mesenchyme.
A. Epidermis
At first, the embryo diilapisi by a single layer of ectoderm cells (Fig. 20.1A). At the beginning of the second month, the epithelium is split and formed a flat layer of cells, or epitrikium periderm, on its surface (Figure 20.1B). In the subsequent cell proliferation in the basal layer, forming a third zone (intermediate zone) (Figure 20.1C). Finally, at the end of the fourth month, the epidermis obtain definitive arrangement, and can be recognized four layers (Fig. 20.1D)

1. Stratum basale or stratum germinativum, play a role in cell menghasiikan new cells. This layer is then
formed ridges and hollows that are reflected on the surface of the skin as a fingerprint.
2. Stratum spinosum thick composed of cells that contain large polihedral tonofibril fine.
3. Stratum granulosum contain small granules keratohialin cells.
4. Stratum corneum (horny layer) that mem ¬ form a hard surface like scales on the epidermis, composed by
dead cells are tightly packed and contain keratin. Periderrn cells are usually released during the second half
of intra-uterine life and can be found in the amniotic fluid. During the first 3 months of development, the
epidermis was invaded by cells derived from neural crest. These cells synthesize the pigment melanin in the
melanosomes. After collection, the melanosomes are transported through the process of the dendritic
melanocytes and transferred to keratinocytes intercellular skin and hair shoots. In this way, skin and hair
pigmentation obtained.
B. dermis
Dermis derived from lateral plate mesoderm and dermatome of the somites. During the third and fourth months, this network, korium (Figure 20. ID), forming many irregular papillary structures, papillae protruding into the dermis to the epidermis Most of these papillae contain capillary smooth or end organ (the tip) sensory nerve. The deeper dermis layer, subkorium, containing many fat tissue.
At birth, the skin covered by white pasta, vernix caseosa; formed by the secretion of the sebaceous glands and hair cells of the epidermis and to the natural degeneration. This layer protects the skin from the amniotic fluid maceration effects.
C. hair
Hair appears as a solid proliferation of epidermis which penetrate the underlying dermis (Figure 20.3A). At the end of the terminal, having the hair bud invagination. Invagination, the hair papilla, quickly filled by mesoderm formation where blood vessels and nerve endings (Fig. 3.20-B, C).
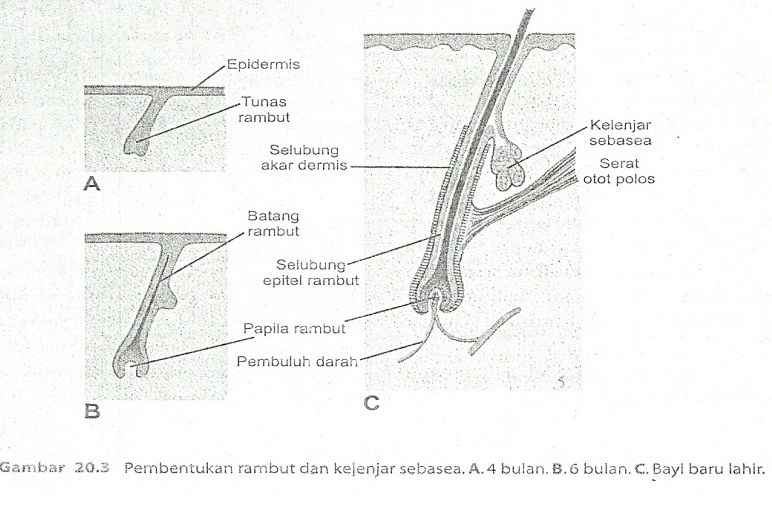
Cells in the central part of the hair bud as soon transform into a spindle and having keratinization, forming the hair shaft, while the peripheral cells become cuboidal and produce hair sheath epithelium (Fig. 20.3B, C).
Dermal root sheath is formed by the surrounding mesenchyme. Root sheath in the dermis is usually attached to a smooth smooth muscle, also derived from the mesenchyme.
These muscles are m. arektor pili. Epithelial cell proliferation continues in the base of the hair shaft pushing the hair up, and at the end of the third month of the first hair has appeared on the surface around the eyebrows and upper lip. The first hair appeared, lanugo hair, loss at birth and later replaced by a more coarse hair that grows out of a new follicle.
Epithelial wall of the hair follicles usually showed a small buds that penetrate surrounding mesoderm (Fig. 20.3C). The cells of these buds form sebaceous glands. The cells of the gland degenerates, forming a fat-like material that is secreted into the hair follicle, from which the material reaches the skin.
D. mammary gland

Early signs of mammary gland was found in the form of elongated thickened epidermis, mammary line or mammary ridge. In the 7-week embryo, these lines run on both sides of the body from the base of the arm to the region of the limb (Figure 20.4C). Although most of the mammary line disappears as soon as formed, a small portion settled in the thoracic region and penetrate the underlying mesenchyme (see Figure 20.4A). In sinij line forming 16 to 24 buds which then produces a small solid buds. At the end of prenatal life, the experience canalization of epithelial buds and form lactiferous ducts, and the buds forming small ducts and alveoli of the gland. At first, the lactiferous ducts open into a small hole epithelium (Fig. 20.4B). Immediately after birth, this hole is turned into a breast due to proliferation of mesenchymal putting underneath.
Skin anatomy
Garus division of the skin is composed of three main layers, namely:
1) layer of the epidermis or cuticle
2) layer of the dermis (Korium, kutis vera, true skin)
3) subcutaneous layer (hypodermic)
There is no middle line which separates the dermis and subcutis, sub kutis characterized by the presence of loose connective tissue and fat cells and tissues.
A. The epidermis or cuticle layer
The epidermis is the thin outer layer of skin and avaskuler. Layered epithelium consists of flattened horns (keratinocytes), the cell contains melanocytes, Langerhans and Merkel. Thick epidermis varies in different parts of the body, the thickest on the palms of the hands and feet. Thickness of the epidermis is only about 5% of the entire thickness of the skin. Regeneration occurs every 4-6 weeks (6).
Layer of epidermis consists of five layers (from top layer to the deepest) 2:
1) the stratum corneum (horn layer)
Outermost skin layer and consists of several layers of flattened cells that die, no core, and protoplasmanya has turned into keratin (horn substance).
2) Stratum Lusidum
There are under a layer of corneum, a layer of flattened cells without a nucleus with the protoplasm is transformed into a protein called eleidin. These layers are more apparent in the palm of the hands and feet (not visible in the thin skin).
3) Stratum granulosum (Layer keratohialin)
Is 2 or 3 layers of flattened cells with coarse grained cytoplasm and nucleus are in between. Coarse grains consist of keretohialin (granule keratohialin). Mucosal layer usually do not have it and it was evident on the palms of the hands and feet.
4) Stratum spinosum (Stratum Malpighian / prickle cell layer)
Consists of several layers of polygonal-shaped cells, the amount varies due to the process of mitosis. Protoplasmanya clear because many contain glycogen, and the core is located in the middle. The cells in the closer to the surface more flattened shape. Among the cells of the stratum spinosum are bridges between cells (intercellular bridges) which consists of protoplasm and tonofibril or keratin. Attachment between these bridges to form a thickening of the small round nodules called bizzozero. Among spinosum cells are Langerhans cells as well. Tues stratum spinosum contain much glycogen.
5) Stratum basale
Consists of a cube-shaped cells (columnar) is arranged vertically at the boundary line as Dermo-epidermal palisade. This layer is the lowest layer of the epidermis. This basal cell mitosis and entered the reproductive function. This layer consists of two cell types, namely:
a. The cells are columnar berbenuk with basophilic protoplasm and large oval nuclei, connected to each other by intercellular bridges.
b. Melanin-forming cells (Melanocytes) or clear cell is a light-colored cells with basophilic cytoplasm and dark nucleus and contains grains of pigment (melanosomes).
Epidermis is renewed every 28 days to migrate to the surface, it depends on the location, age and other factors.

B. The dermis layer
The most important part in the skin that is often considered a "True Skin". Is the thickest layer of the dermis can be found in the back and thinnest on the palpebrae. The relationship between the dermis and the epidermis is not as flat field, but the shape of the wave. Parts that protrude into the dermis called papillae epidermis, while the epidermis into the dermis called prominent rete ridge. These papillae on the palms and fingers are composed mainly of linear which gives an overview of different skin as dermatoglyphic (fingerprint). This part of the papillary dermis thickness about one-fifth of the total dermal thickness. The lower part of the papillary dermis is called the reticular dermis containing blood and vasa lymphe, nerve fibers, and other adnexa (7).
The dermis is composed of several elements or organs which include: elements of cellular, fibrous elements, the basic substance, and limphe blood vessels, nervous system.
1. More mobile elements found in the papillary stratum consisting of:
a) fibroblasts: an element for forming fibrous cells and basic substance
b) The cell degranulation: a cell-forming and storage of histamine and histamine like substance that plays a role in anaphylaxis.
c) Macrophages: phagocytic cells that function is memfagosit foreign substances fan of microorganisms.
d) Leukocytes: A lot found in inflammatory processes which can be mononuclear or granulocytes.
2. More dense fibrous elements in the reticular stratum than in the papillary stratum. Fibrous elements consist of:
a) Collagen: is 70% of the dry weight of all connective tissue, fibers are formed by fibroblasts, composed of fibrin from the polypeptide chain. These fibers are responsible for the skin tension lines forming elements Langer (cleavage line)
b) Elastin: Only 2% of dry weight tissue. Elastin fibers, was also formed by fibroblasts, but its structure is more subtle disbandingkan with collagen. Elastin fibers are responsible for skin elasticity.
c) reticuline: collagen fibers is still young and can only be viewed with a special dye.
3. Basic substance, composed of materials mukopolisakaris (hyaluronic acid and dermatan sulfate), which is also formed by fibroblasts. This outcome is only 0.1% of dry weight tissue, but the basic substance is capable of holding some water, so that will occupy the largest space of the dermis.
4. Blood and lymph vessels:
In the skin that is normal, that blood until the skin is 10% of all blood circulation in the body. Blood vessels in the skin plexus is composed of 2:
a) Plexus superficial: there is in the upper dermis and are arranged parallel to the epidermis. Superficial plexus consists of the kepiler-capillary, a member venulae endarteriole and fed into the papilla.
b) The deep Plexus: There are at or near the bottom of the dermis and subcutis mainly consists of blood vessels larger than the superficial plexus.
Nervous system
Skin innervated by approximately one million afferent nerve fibers. Mostly found on the face and extremities, while the back is relatively small. These nerve fibers had axons with cell bodies located in the dorsal root ganglia. These nerve fibers enter the skin through the subcutaneous fat layer, then each is two bermyelin nerve fibers and nerve fibers are not bermyelin. Bermyelin nerve fibers run horizontally woven with the fibers forming the same, then ascending up along blood vessels and the superficial dermis menginervasi. In subsequent trips fibers are wrapped by Schwann cells and some did not bermyelin. Partly end up in the dermis, some penetrating the basal membrane but did not continue far into the epidermis.
There are three kinds of nerve fibers found on the skin yag, namely:
1. Adrenergic fibers: for menginervasi vascular function (to vasoconstriction of blood vessels, erector papilare m (for muscle contraction), and apocrine glands (apocrine gland secretion for the regulator.
2. Cholinergic fibers: menginervasi gland function ekrin.
3. Sensory fibers: function to receive stimuli from outside the body. There are multiple endings of sensory nerve fibers, namely:
1) Korpuskulum Meisnerri
Serves to receive a light touch and pressure stimuli. Papillae present in the dermis and most can be found on the palms of the hands and feet.
2) Korpuskulum Paccini
Serves to receive the stimulus and there is pressure in the inner dermis, especially in parts of the body that often hold heavy loads.
3) free nerve fiber endings
Serves to receive the stimulus of heat, cold, pain, itching. Free nerve endings are found mainly in the papillary dermis and around hair follicles.
Boundary between the epidermis and dermis is formed by the basement membrane zone. By using the electron microscope, this membrane can be composed of 4 components: cell membrane of basal cells with hemidesmosom, intermembranous gap, basal lamina, fibrous components of the dermis can be seen with an ordinary microscope with a special dye using PAS. Basement membrane zone is a semipermeable filter which allows the exchange of cells between the dermis and dn epidermis2 fluid.
The dermis functions: structural support, mechanical strength, the supply of nutrients, resist shearing forces and the response inflamasi6.
C. Subcutaneous layer
A layer below the dermis or consisting of hypodermic fat layer. This layer of connective tissue that connects there is a loose skin with underlying tissues. The number and size vary according to where the body and the circumstances of individual nutrients. Serves to support the blood supply to the dermis for regeneration.
Function subcutis / hypodermic: attached to the base structure, thermal insulation, spare calories, shape control and mechanical shock absorber (6).
vascularization of skin
Arteries that nourish the skin form a plexus located between the papillary and reticular dermis layer and in addition between the dermis and subcutaneous tissue. Small branches leave this plexus memperdarahi dermis papilla, each papilla dermis had one artery and one branch ascending vein. In the epidermis there are no blood vessels but gets nutrients from the dermis through epidermis membrane (6).

Skin Physiology
The skin is an organ that functions essential for the body of which it is possible to survive in various environmental conditions, as a barrier to infection, control of body temperature (thermoregulation), sensation, eskresi and metabolism.Protection function is to protect the skin from the loss of fluid from the electrolyte, mechanical trauma, ultraviolet, and as a barrier to invasion of pathogenic microorganisms. The sensation is one of the known functions of the skin in response to touch stimuli such as the number of nerve endings in the lips, nipples and fingers. Role in the regulation of skin temperature and fluid electrolyte balance. Thermoregulation is controlled by the hypothalamus. Peripheral temperature undergo a process of balance through sweat, insessible loss of skin, lung and buccal mucosa. Skin temperature is controlled by dilating blood vessels or skin kontriksi. When the temperature rise occurs vasodilatation of blood vessels, then the body will reduce the temperature by removing heat from the skin by sending a chemical signal that can increase blood flow in the skin. In the temperature decreases, the skin will be vasoconstriction of blood vessels which then would retain heat (6)
Classification of Malignant Skin Tumors
Malignant skin tumors are most commonly found are:
1. Basal Cell Carcinoma
2. Squamous Cell Carcinoma
3. Malignant tumors (malignant melanoma)
A. BASAL CELL CARCINOMA
Definition
Basal Cell Carcinoma (BCC) is a malignant neoplasm of epithelial cells is more like a set germmatif hair follicles compared with the basal cell layer of the epidermis. KSB is fibroepitelial tumor stroma composed of interdependent components of the base (fibrous tissue) and epithelial. Tumor cells derived from primordial pluropofensial in basal cell layer, and may also from outside the root sheath of hair follicles or sebaceous glands or skin adnexal lain.5
Another name for Basal Cell Carcinoma is Basalioma noodles, Basal cell L-pitellioma. rodens ulcer. Jacob ulcer, tumor komprecher, basal cell carcinoma.
Epidemiology
First of all the reported Basal Cell Carcinoma This is Jacob in 1827 that meruapakan a cell invasion and metastasis are slow, and rarely cause kematian.5 Basal Cell Carcinoma is more common in whites than in people of color and light effects the sun was instrumental in the development of Basal Cell Carcinoma. More men than in women and generally over 40 years. More than 80% are located in the head and neck, 30% in the nose.
According to research in Indonesia Tjarta ranking of skin cancer are:
1. Basal Cell Carcinoma 36.67%
2. Squamous Cell Carcinoma of 11.4%
3. Malignant melanoma is 0.59%
4. Malignant adnexal tumors of skin and other skin malignant tumor
Predisposing factors of Basal Cell Carcinoma
1. Internal factors: age, race, gender, and genetic
2. External factors
1. UV rays (UVB 290 -320 um)
2. Trauma to the skin sepeni vaccination scars, burns
3. Chemicals, polycyclic hydrocarbons
4. Radiation lonisasi
5. Organic arsenic
Pathogenesis
Pathogenesis of Basal cell carcinoma is often preceded by the collagen found in skin pigments and gets a little excessive sun so that impaired nutrition of the epidermis where it is a predilection for the occurrence of an abnormality kulit.8 Melanin serves as an amorphous energy that can absorb energy and eliminate them in the form If the incoming heat energy is too large and can damage or kill cells mutate into cancer cells to selanjulnya.
Clinical manifestations
Predileksinya especially on the face (pipi. forehead, nose, fold, nasolabial, periorbital area), the neck. Although rare can also be found on the arms, Langan, body, legs, feet, and leather palm. These tumors grow slowly and rarely distant metastasis, but tend to be locally invasive and cause severe morbidity, local rekurrensi and tissue destruction. Metastasis may occur in the so-called nodular variant of basal cell carcinoma basaloskuamous.
Clinical picture at variance KSB, KSB Lever divide into 5 forms
1. Nodulo-ulcerative, including ulcers rodens
2. Pigmented
3. Morfea or fibrosing or sklerosing
4. Superficial
5. Fibroepitelioma
Is the type most often encountered. Lesions usually appear as single lesions most commonly on the face, especially cheeks, nasolabial fold. forehead, and eyelid edge Initially lampak papule or small nodule, transparent like a pearl. diameter less than 2 cm, with a rising edge. The surface looks sleek. teleangiektasia common presence. and sometimes with a smooth or a crusting skuama thin. Colored like pearls, sometimes like a normal skin to a pale erythematous. Lesion enlarged slowly and one day the center of the lesion to be concave, the rising edge of the hard left. If neglected, these lesions will ulcerated (called ulcers rodem), with tissue destruction in Had

Pigmented type
Clinical picture similar to the type of ulcerative nodulo difference, in this kind of brown or black colored speckled or homogeneous Minis that can resemble melanoma.

Type Morfea fibrosing / Sklerosing
Usually occurs in the head and neck lesions appear as a concave sclerotic plaques. yellowish white with unclear boundaries. Growth was followed by the expansion of peripheral sclerosis in the middle.

Superficial type
Lesions are usually multiple, the body appears as a plaque Minis In transparent, eritematousa until light pigmented, oval-shaped with irregular edges of bounded sarnpai legas slightly elevated, such as thread or wire. Usually associated with chronic arsenic digestion

Type Fibroepitelial
Most common in the lower back Clinically, the lesions of small papules that are not stemmed or short stemmed. with a smooth surface with varying warm.
Histopathology
Lever divided in several types histopalologi KSB comprising KSB KSB differentiated and undifferentiated.
1. KSB differentiated
a. Types of keratotic
Also called type pillar therefore differentiate toward hair cells show a picture parakeratotik with elongated nuclei and slightly eosinophilic cytoplasm and found horncyst, besides undiferentiated cells with basophilic cytoplasm
b. Types of cystic
Found the parts in the middle cystic tumor mass caused by the degeneration of tumor cells or cells defferensiasi to the gland.
c. Type of adenoid
A picture of the gland-like structures that are restricted Sometimes the connective tissue is found that lumen dikeilingi bersekresi cells. Such can be found in the lumen of colloidal materials or amorphous mass.
2. KSB does not differentiate / BCC solid
Histopathologic picture is commonly found. Form islands of cells with the shape and size vary, composed of basaloid cells, with basophilic nuclei which bulal or oval. little cytoplasm, the cells at the edge of the tumor mass composed of palisade.
Diagnosis
Complaints generally are lesions such as moles that enlarge, may also be in the form of ulcerative lesions that do not heal. Gambaan classic known as rodent ulcers are ulcers with uneven edges, blackish color with visible peripheral hyperplasia (rising) and the central ulcer. Classical form does not vary depending on the type klinikkopatologinya. At the beginning of basal cell carcinoma was found generally small, translucent or pearly, was an area that stands out in the presence of dilated blood vessels (telangiectasia). Growth is slow, but if neglected can grow into the deeper skin layers and cause great damage, especially basal cell carcinoma growing in the area around the eyes, nose, or ears.
Basalioma usually a papule lesions, nodules, translucent pearl, ulcers (often covered with crusts) with raised edges, pink or red, telangiektasis can be found (with the help Loupe). This type can be pigmented brown to blue or black. On palpation can be felt hard, solid and cystic. Shape is usually round, oval, curved center (umbilicated). Almost never obtained metastasis to regional lymph nodes. Diagnosis must be confirmed by examination histopatologi.13
Management
Management of KSB aims to obtain healing with good cosmetic results and functional outcomes are maximized. In determining how the management of BCC, many things to consider, from both tumor and patient factors. Tumor factor to consider is the type of tumor, the size of the location, nature of the primary tumor growth and whether or rekurens. While patient factors to consider are age, history of other diseases, psychological factors and medical history.
Broadly speaking, the management of BCC is classified into 2 groups, ie with and without surgery surgery Surgery may be done by excision with skapel, Mote mikrografik surgery, curettage and elektrodesikasi, frozen surgical and nonsurgical management of laser surgery performed by means of radiotherapy, intralesional interferon, chemotherapy. retinoid administration and dynamic images.
Prognosis
KSB provide treatment in primary cure rate of about 95% whereas in KSB Recurrent about 92%. Treatment of recurrent KSB KSB is more difficult than the primary, and the recurrence rate as tired as do the second procedure is high.
2. Squamous Cell Carcinoma
Definition
Squamous cell carcinoma is a malignant proliferation of keratosit epidermis, which is an epidermal cell types of the most widely and is one of the common skin cancer after basalioma. Predisposing factors of squamous cell carcinoma (SCC), among others, ultraviolet radiation, carcinogenic materials. arsenic and other lain.9
KSS is another name for squamous cell epitheliomatous (prickle), prickle cell carcinoma, epidermoid carcinoma, pavement epithelioma, spinalioma, Bowen carcinoma and epithelioma cormfied. 2
Epidemiology
SCC is more common in whites than in skin color and more common in men than women, especially at the age of 40-5 - years. SCC incidence rises with age setting 9
Etiology
Like most other cancers, the cause of skin cancer is also not known for certain There are many factors that can cause the growth of SCC of the skin to sunlight is a factor, arsenic, hydrocarbons, temperature, radiation, chronic, scarring, virus.8
The role of UV for skuamousa cell carcinoma through various mechanisms. UV-B appear to affect the density and the capability of Langerhans cells of interleukin-2 (T helper 1 cytokine) and interferon. Research has proved that ultraviolet rays to the introduction of mutations of p53 by producing pyrimidine dimers from DNA can therefore be considered that the ultraviolet light as a trigger marker mutasi.13
Manefestasi Kllinik
KSS in general often occurs at the age of 40-50 years with the most common location is the area most exposed to the sun such as face, ears, lower lip, back, hands and lower limbs.
Clinically there are two forms of SCC, namely
1. SCC in situ
Squamous cell carcinoma is confined to the epidermis and occur in a variety of skin lesions that have been there before as solar keratosis, chronic radiation keratosis, hydrocarbon keratosis, keratosis arsenikal. cornua cutanea. Bowen disease, and SCC in situ entroplasia Queyrat can be settled in the epidermis in the long term and unpredictable. can penetrate to the basal layer of the dermis and subsequent metastasis via the lymphatic channels of the region.

2. Invasive SCC
Invasive SCC may develop from the KSS in situ and may also from normal skin, although jararang either early invasive SCC arising in karsinorna in situ, premalignant lesions or normal skin, usually in the form of small nodules with no apparent boundary, stained with skin color or slightly less erythema surface at first gently and then developed into papilomatosa verukosa or ulceration usually occurs near the center of the tumor, it can happen sooner or later, the string before the tumor diameter of 1-2 cm. Granular surface of the tumor and may bleed easily, while the edge of the ulcer is usually elevated and hardened. Can be found crusting 8.10

Stadium Clinic
Clinical staging for basal cell carcinoma (basiloma) and squamous cell carcinomas using standard TNM-AJCC (American Joint Commission on Cancer) 2002.

Histopathological
KSS histopathologically composed of irregular masses of epidermal cells that proliferate and invade into the dermis well-differentiated SCC showed the rapid keratinization of squamous cell layers of tumor cells arranged in a focal and concentric with the mass of keratin, forming horn pearls (hom pearls) that are characteristic of well differentiated SCC.
In the poorly differentiated SCC showed keratinization is limited or atypical cells with abnormal mitosis picture. Intercellular bridges are not found.
Diagnosis
The main complaint is that the skin lesions grew prominent, easy bleeding, ulcers such as the top there is cauliflower with a characteristic odor. On physical examination found lesions that grow eksofitik, grew progressively and sometimes bleed easily be ulkud with a characteristic odor.
Squamous cell carcinoma usually grows first in the form of keratotic patches and become nodules eritematos further heightened by the ulcer, with a crust of keratinized, horned with a rising edge, wet, and smells of a typical bleed easily. KSS is often associated with subcutaneous extensions that can cause damage to the dermis layer, which may be associated with the onset of pain because they perineural invasion. Clinically suspected squamous cell carcinoma when there is a lesion on the skin, especially on sun-exposed skin or trauma, betuk plaque, nodules, papules, tumors or ulcers, bleed easily, solid consistency, there is growing eksofitik, endofitik, infltrat rapidly progressive. 13 Definitive diagnosis is by histopathological examination. 4.8
Management
KSS and treatment depends on tumor size, shape and location of tumor, the nature of the skin where the tumor arises, type. diinvsi depth of the tumor tissue.
In the squamous cell carcinoma of the incision limits the diajurkan adalah1-2 cm beyond the induration. If there are metastases to regional lymph nodes, should be performed lymph node dissection that is modified neck dissection, the superficial inguinal node dissection or axillary dissection to level II. Specifically squamous cell carcinoma of the skin on the head and neck dissection is recommended that classic radical neck dissection because of cancer is very limfogenik and infiltrating.
Treatment according to stage, stage I, II, and III (T4 N0 M0 with) performed wide excision with 1-2cm incision boundary. Stage III (with T1, N1 M0 2.3) performed wide excision and regional lymph node dissection. Stage IV were given only palliative therapy.
Primary radiation is indicated in inoperable cases, cases with poor operation tolerance and the patient refused surgery. Adjuvant radiation is given on the condition: tumor-free limits not incision, the incision near the tumor boundary, there is contamination of the operating field by tumor cells and radicalism incision in doubt.
Lokoregional adjuvant radiation to be given if lymph nodes contain more than one metastasis, lymph node diameter> 3 cm, there is an extra capsule growth or high grade malignancy. Radiotherapy should be avoided in younger patients because of the long-term cosmetic morbidity and risk for squamous cell carcinoma in the radiation area.
Primary chemotherapy is indicated in cases with distant metastases, inoperable or patients who failed treatment with surgery and radiotherapy. Chemotherapy is commonly used is cisplatin, 5-fluorouracil, bleomycin and doxorubicin.
70% -80% of all skin SCC rekurrent in the first 2 years after surgery. Therefore, strict follow up on this very crucial period.
2. Malignant Tumor (malignant melanoma)
Definition
Skin is a malignant tumor derived from melanocytes with an overview of sd blackish lesions on the skin of unknown cause is common in the age of 30 to 60 Tahua equal frequency in men and wanita.8
Various factors are thought to be an important factor in the mechanism of carcinogenesis of malignancy is as follows.
1. Genetic factors
Family is suffering from this malignancy increases the risk of contracting malignant melanoma 200 times. Familial malignant melanoma was found in 8% of new cases of malignant melanoma occurrence jug teriadinya didihubungkan with other malignancies such as retinoblastoma and some malignant syndrome in a family.
2. Melanocytic nevi
This situation may arise related to a genetic disorder or a certain environment. The number of nevi were found related to the amount of sun exposure in childhood and the presence of certain genetic defects. A number of malignant melanoma occur 30-90% of pre-existing nevi.
3. Biological Factors
Prolonged trauma is a risk of this malignancy. for example, the irritation caused by a belt. Other biological circumstances that affect the immunological resistance is reduced. for example in patients with kidney removal and also M. Hodgkin's malignant melanoma will memngkatkan events. Changes in hormonal state also increased the incidence of malignant melanoma and also meningkalkan relapse after treatment in patients with malignant melanoma
4. Environmental factors
Exposure to UV rays from the sun is an important factor associated with an increased occurrence of malignant melanoma, especially if there is sun burn repeated low in people with pigmented symptoms and specific signs are found in malignant melanoma that has been widely known. is as beriku (ABCDEF from malignant melanoma)
A merry-Sy, the rumors are not symmetrical shape
Border Irregularity, that is the boundary line that does not teralur
Colour variation, from colorless to black in a single lesion.
tumor diameter greater than 6mm
Evolution / change of the lesion can be considered by the patient or family.
Funny looking lesions

Manefestasi Clinic
There are three types of malignant melanoma (Clark, 1967.1969 and Me Govern, 1970) with I type a new lambahan (Reed, 1976 and Seiji, M, et al. 1977). These four types of malignant melanoma is composed of:
1. Superficial spreading melanoma (SSM)
Is the largest type of melanoma (70%) in Indonesia is the second largest type. Generally arise from the nerve or the normal kulil (de novo), Form of plaque size from 0.5 to 3 cm archiformis with lepi elevated and irregular. At permukaamya are a mixture of various colors. like chocolate. gray, blue. black and often reddish. Extends generally radially Tesi 2 cm in size within 1 year. to continue to grow vertically and develop into a blue-black nodules regressed Dapal sponian by leaving patches of hypopigmentation. Predileksinya in women encountered in the lower leg, while the men in the body and neck.

Epidermis: - Melanocytes berbenluk epithelioid, can be arranged individually or in groups
- In general, these cells did not show the shape of a pleomorphic
Dermis : - nests of solid tumors by large epithelioid-shaped melanocytes and atypical berkromatin
- Inside the cells there are grains of melanin
- Sometimes the spindle-shaped melanocytes can be found (spindles) and inflammatory cells
2. Nodular Melanoma (NM)
Jeras melanoma is the second largest (15-30%) sifalnya Icbih aggressively in Indonesia is the type lersering noodles. Arise on normal skin (de novo) and rare form of nevus and a half bulb-shaped nodules (dome shaped), or polypoid and eksofitik, berwarra kemerahana brown or blue to black growth is vertical (invasive) can be ulcerated. bleeding, and lesions arising salelit limfogen Metastasis and hemalogen, may arise from the beginning mainly found in men with prediteksi dipunggung. Comparison between men and women 2:1.

Epidermis: - Melanocytes epithelioid and spindle-shaped or a mixture of both forms tersebul. can in the
Dermo
Dermis: - From the beginning, these cells have the ability to expand vertically. Retikularisdermis
invaded layer, blood vessels and subkulis
3. Lentigo Malignant Melanoma (LML)
this lesion is rare (4-10%).
Vertical growth. very lambal with most locations in the area of the exposed face of the sun
Arising from hutchinaon's freckle found on the face (cheeks, temples) or in other parts of the body especially sun-exposed areas that form of macular brown to black, measuring several centimeters with irregular edges. Expanding slowly on the edge of the lesion (radial) On the surface dapal found the patches of the darker colored (black) or blue, are scattered irregularly to develop into blue-black nodules that are invasive and somewhat hyperkeratotic mainly found in older women Comparison between men and women 1: 2-3.

Epidermis: - Melanocytes atifik basalts along the membrane, forming pleomorphic with atypical nuclei.
- The cells are frequently encountered form of a coil (spindleshaped melanocyl)
Dermis: - Intilirasi lymphocytes and macrophages containing melanin.
- Occasionally found in certain places the tumor nests.
4. LeMiginous Acral Melanoma (ALM) / Palmar-Plantar-Subungual Melanoma (PPSM)
Generally arise on normal skin (de novo).
Form nodules with varying colors and on its surface arise dapal papules, nodules and ulcerations. Sometimes the lesions do not contain pigment (amelanotic melanoma).
Predileksinya: on the soles, heels, palms, nail beds, teruiama toes and hands

Is the type that is prevalent in African and other nations who live in the tropics In Afnka. plantar melanoma is found in 70% of cases.
Lentinginous Acral Melanoma (ALM) is a type more commonly found in people of color (35-60%). Resembling a picture of malignant melanoma, SSM. or a mixture of both
Clinical Systems
In the classification system used malignant melanoma clinic (clinical stage) and histological classification (Clark level of invasion and Breslow depth) 3,4,5,6,9,
Usefulness or importance of classification systems, namely:
To determine iindakan treatment.
To determine the prognosis.
To compare treatment outcomes between the various clinics
Classification Clinic
Until now used Stadium Clinic (with some modifications) as the standard classification of malignant melanoma, consisting of 3 stadium6, 8,11,12
Stage I: malignant melanoma without distant metastases or local to regional lymph nodes.
Including stage 1:
Primary melanoma untreated or tdah excision biopsy is performed.
Melanoma local recurrences that are within 4 soitimeter of
primary lesion
Multiple primary melanomas.
Stage II: There has been limited metastatic regional lymph nodes.
Includes Stage II.
Melanomap rimer who hold metastasis simultaneously.
Terkortrol primary melanoma and metastases occur later.
Local recurrences with metastatic melanoma.
In-transit metastases that are beyond a distance of 4 inches from the primary lesion.
Melanoma of unknown primary with metastasis
Stage III: Melanomad iseminala, where distant metastasis has occurred.
Including Stage III
If metastasis has occurred to the tools and or subcutaneous.
In approximately 25-30% of patients with malignant melanoma has metastasized to indicate the presence of regional lymph nodes, although not clinically palpable lymph node enlargement. This explains that in order to determine the prognosis and treatment measures are not enough to just be based on the classification Stadium Clinic, but need to be accompanied and determined based on histological.
Classification of histological
Histologic classification based on biological temperament malignant melanoma. Are two standard histological klasifikai used, namely .8,11,12
• Classification lingkat invasion according to Clark
• Classification according to Breslow depth
Klasifikai The Invasion According to Clark
Clark (1969) divided by the invasion of malignant melanoma in the skin of five tingkat8, 11.12
Rate: Tues melanoma located above the basal membrane of the epidermis (melanoma in situ: intraepidermal) is very rare and do not harm:
Level II: Invasion of melanoma cells to the papillary layer of dermis (the superficial dermis).
Level III: Invasion of melanoma cells to the border between layers of papillary and reticular dermis layer of the melanoma cells fill the dermis papillae.
Level IV: The invasion of melanoma cells to the reticular layer of dermis.
Level V: Invasion of melanoma cells to subcutaneous janngan

Classification of depth (thickness) of tumor according to Breslow
Breslow (1970) divides into three golongan2 malignant melanoma, 4,5,6,9,
Group I: The depth (thickness) of less than 0.76 mm tumor
Class II: The depth (thickness) of tumors between 0.76 mm - 1, 5mm
Group III: With the depth (thickness) of greater than 1.5 mm
Some authors propose vanasi as follows:
The depth (thickness) mm 4 0.85 kurangdari tumor
The depth (thickness) of tumors between 0.85 mm - 1.69 mm.
The depth (thickness) of tumors between 1.70 mm-3.64 mm.
The depth (thickness) of greater than 3.65 mm.
Depth (thickness) of tumor according to Breslow, measured directly using a micrometer eyepiece (expressed in NM) and an objective method for determining the prognosis. While the level of invasion according to Clark is the measurement of tumor thickness indirectly. The relationship between the level according to Clark and depth (thickness) according to Breslow tumor: malignant melanoma with a depth of up to 0.65 mm according to Breslow classification, in accordance with the Level II according to klasifikai Clark. Malignant melanoma lesions with a depth of 1.5 mm or more by klasifikai Breslow, in accordance with tingkal IV and V according to Clark's classification, while a depth between 0.65 mm and 1.5 mm according to the classification of Clark.
Diagnosis is by biopsy to remove all the suspicious growth. If the network is too large to be appointed. then simply removed any tissue sample.
Management include:
A. Eksist surgery.
Performed on melanoma stage I and II Zitelli et al Suggest to pick up to 1.5 cm beyond the edge lesinva, except when done Moh's microsurgery. At present melanoma of the nail is recommended to do an amputation on all the affected finger.
B. Elective lymph node Dessection (ELND)
Performed in stage III melanoma, where there has been metastasis to the lymph glands. This is evidenced by a palpable enlargement of lymph glands ELND remains a controversial treatment is the preferred way is by intraoperative lymphatic mapping.
C. Interferon a-2b
Can be used as an adjuvant therapy in melanoma is larger than 4 mm (stage V), but should still be considered a high level of toxicity. The goal is expected to inhibit metastasis further.
D. Chemotherapy
Said to be not very useful in the treatment of melanoma is the most effective type of chemotherapy is dacarbazine (DT1C-Dimethyl Triazone Imidazofe Carboxamidc Decarb zine).
E. Perfusion Chemotherapy
This method aims to create an atmosphere pembulun hipertermis and oxygenation in blood vessels in tumor cells and limit the distribution kemotlerapi using torniquet
This method is expected to replace the amputation as a treatment.
F. Radiation Therapy
Used only as a symptomatic therapy in melanoma with metastasis to the bone and central nervous system (CNS). Nevertheless the results are not so satisfactory.
Without treatment, most metastatic melanoma and will result in patient death. At present, because the clinical diagnosis is dim. more than 80% of melanoma were treated with simple surgical exist and with better education about the clinical signs of melanoma, a 95% recovery rate.
CONCLUSION
1. Malignant skin tumors are malignant process arising from the surface of the skin and epithelial cells, or cells pluripotensial of melanin in the skin cells.
2. According to a differentiated cell type, malignant skin tumors were classified as follows: basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and malignant melanoma (MM).
3. According to etiology, malignant skin tumors can be caused by (1) extrinsic factors of exposure to ultraviolet light, X-ray exposure, the use of chemicals and the presence of extensive scar tissue and old, (2) of intrinsic genetic factors, low immune system and race .
4. Basal cell carcinoma is usually found on the face and neck with clinical symptoms of ulcerative nodules, pigmented, morfea, superficial and fibroepitelioma. Usually characterized by a rising edge of the ulcer in the absence of distant metastases.
5. Predilection for squamous cell carcinoma on the sun-exposed skin and mucous membranes with the clinical picture in the form:
(1) normal skin-colored nodule with a smooth surface without crusting.
(2) reddish nodules with surface papilomatosa / verukosa cabbage-like relationship.
(3) ulcer with crusting on the surface with the rising edge of reddish yellow.
6. Malignant melanoma most often grows in sun-exposed skin, but almost half the growth of pigmented moles, there are signs of inflammation in the skin around the mole, it changes color, size, shape / consistency of distant metastases as well as easy to hold.
7. Diagnosis of malignant skin tumors is based on symptoms and clinical investigation.
8. BCC and SCC treatment is usually to remove the tumor, either by curettage and elektrodesikasi and cut with a scalpel. While the MM treatment principle is to perform an excision that was originally carried out measurements of the thickness of the first invasion by the Breslow thickness technique.
9. Prognosis of KSB is a good cure rate skitar 95% whereas in SCC varies depending on location, size, degree of differentiation of the cells and the depth extension, and in MM prognosis is determined by the nature of the tumor, clinical stage, location of metastases and patient factors.
REFERENCES
1. Djuanda. A., Hamzah. M., Aisah. S., 1999. Ilmu Penyakit Kulit dan Kelamin, Tumor Kulit, Melanoma Maligna, edisi 3 Bagian Ilmu Penyakit Kulit dan Kelamin FKUI, Jakarta.
2. Lim Pei-wen, Sharen, 2008. Kanker Kulit. Diakses dari http://wikipedia.org/kanker_kulit.htm
3. Agung, Gusti, 1985. Tumor Ganas Dini Kulit. Cermin Dunia Kedokteran. FKUI, Rumah Sakit Cipto Mangunkusumo, Jakarta.
4. Anonim, 2006. Mengenal Kanker Kulit. Diakses dari http://www.dharmais.co.id
5. Perdanakusuma, David, 2008. Anatomi Fisiologi Kulit dan Penyembuhan Luka. Diakses dari http:// surabayaplasticsurgery.blogspot.com/2008/05/ anatomi-fisiologi-kulit-dan-penyembuhan.html
6. Price, Wilson, 1995. Patofisiologi, Konsep Klinis Proses-proses Penyakit. EGC, Jakarta.
7. Graham, R. 2005. Lecture Notes on Dermatologi. Ed. 8. Jakarta: Erlangga
8. Anonim, 2006. Nutrisi Pada Penderita Kanker Kulit. Diakses www dharmais co id
This comment has been removed by the author.
ReplyDeleteThere are some natural remedies that can be used in the prevention and eliminate diabetes totally. However, the single most important aspect of a diabetes control plan is adopting a wholesome lifestyle Inner Peace, Nutritious and Healthy Diet, and Regular Physical Exercise. A state of inner peace and self-contentment is essential to enjoying a good physical health and overall well-being. The inner peace and self contentment is a just a state of mind.People with diabetes diseases often use complementary and alternative medicine. I diagnosed diabetes in 2010. Was at work feeling unusually tired and sleepy. I borrowed a cyclometer from a co-worker and tested at 760. Went immediately to my doctor and he gave me prescriptions like: Insulin ,Sulfonamides,Thiazolidinediones but Could not get the cure rather to reduce the pain but bring back the pain again. i found a woman testimony name Comfort online how Dr Akhigbe cure her HIV and I also contacted the doctor and after I took his medication as instructed, I am now completely free from diabetes by doctor Akhigbe herbal medicine.So diabetes patients reading this testimony to contact his email drrealakhigbe@gmail.com or his Number +2348142454860 He also use his herbal herbs to diseases like:SPIDER BITE, SCHIZOPHRENIA, LUPUS,EXTERNAL INFECTION, COMMON COLD, JOINT PAIN, EPILEPSY,STROKE,TUBERCULOSIS ,STOMACH DISEASE. ECZEMA, GOUT, PROGENITOR, EATING DISORDER, LOWER RESPIRATORY INFECTION, DIABETICS,HERPES,HIV/AIDS, ;ALS, CANCER , TUMOR, VIGOUR, HALITOSIS, MENINGITIS, WAIST PAIN ,HEPATITIS A AND B,ASTHMA, HEART DISEASE, CHRONIC DISEASE. NAUSEA VOMITING OR DIARRHEA,KIDNEY DISEASE. HEARING LOSSDr Akhigbe is a good man and he heal anybody that comes to him. here is email drrealakhigbe@gmail.com and his Number +2349010754824
ReplyDelete